

Lipid Logic | Ep. 1014
The Next Era of Cardiometabolic Therapeutics
Hello Avatar! Welcome back for another week of biotech analysis. Today is Sunday, which means this is our Building Biotech newsletter that is focused on discussing biopharma strategy topics. This week, we dive into a therapeutic shift that’s quietly redefining lipid medicine. For years, the conversation centered on LDL cholesterol. But as new data emerge, a different culprit is coming into focus: triglyceride-rich lipoproteins and their remnants. Drugs targeting the lipase axis (ApoCIII, ANGPTL3/4/8, and FGF-21) are pushing beyond biochemical endpoints to tackle pancreatitis, atherosclerosis, and MASH at their metabolic root. In this issue, we unpack the science, the clinical momentum, and the companies best positioned to lead in a post-statin world.
We are now publishing 7x per week according to the following cadence:
Mondays: Stocks
Tuesdays: Biotech
Wednesdays: Podcast
Thursdays: Markets
Fridays: News
Saturdays: Podcast
Sundays: Strategy
We are also publishing unique content on X - be sure to follow up if you are not already @BowTiedBiotech. And to check-out the archive of our work on X you can find it on our website at: BowtiedBiotech.subtack.com/x-articles.
SUBSCRIBE TO PODCAST HERE:
Please help spread the work by subscribing and hitting the share button if you are enjoying our bi-weekly newsletters!

Enough shilling for the day, lots to cover this week, let's get started!
Introduction: When Cholesterol Isn't the Only Culprit
For decades, the focus in cardiometabolic disease has revolved around LDL cholesterol. Statins, PCSK9 inhibitors, and ezetimibe reshaped the landscape. But beneath the surface lies another class of particles (triglyceride-rich lipoproteins and their remnants) that drive inflammation, insulin resistance, and organ damage in their own right. These are not just silent passengers in the bloodstream. They’re active saboteurs.
These aren't your classic statins or PCSK9 inhibitors. They don’t reduce production or absorption. They restore clearance. It's biology that’s cleaner, more targeted, and tuned to the root dysfunction. The clearest signals so far are in hypertriglyceridemia, pancreatitis, and fatty liver, but the underlying theme is broader: remnant cholesterol, insulin resistance, and tissue inflammation all start upstream with poor lipid partitioning.
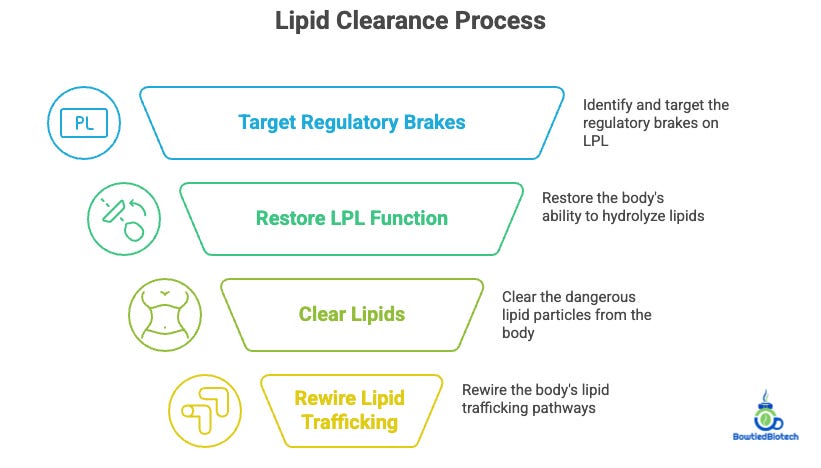
What’s emerging now is a therapeutic framework that targets the regulatory brakes on lipoprotein lipase (LPL), the enzyme responsible for clearing these dangerous particles. Instead of simply blocking production or absorption, these new agents restore the body’s ability to hydrolyze, clear, and rewire lipid trafficking. And in doing so, they offer new hope across three pathologies that rarely intersect in the same treatment playbook: acute pancreatitis, atherosclerosis, and steatohepatitis.
The therapies in question (ApoCIII inhibitors, ANGPTL3/4/8 inhibitors, and FGF-21 analogue) share a common thread: they each increase clearance of triglycerides, either directly through LPL or indirectly by modulating hepatic lipid metabolism.
Together, they represent a new axis in cardiometabolic disease. The question is not whether they work, but where, in whom, and how soon we’ll see outcomes that justify adoption.

Lipoprotein Lipase: The Forgotten Switch
LPL sits at a metabolic crossroads. It hydrolyzes triglycerides from circulating lipoproteins, releasing free fatty acids for uptake by muscle, adipose, and other tissues. But its activity is tightly regulated (by proteins like ApoCIII, ANGPTL3, ANGPTL4, and ANGPTL8) which act like dimmer switches, dialing lipolysis up or down depending on nutritional state and tissue context.
The therapeutic logic is simple: inhibit these brakes, and LPL activity surges. That reduces plasma triglycerides, shrinks remnants, and potentially lowers inflammatory burden in the vasculature and pancreas. But biology rarely rewards simplicity. Each regulator has distinct expression patterns, tissue selectivity, and off-target liabilities. That’s where the recent wave of precision therapeutics enters.
Today, we’re seeing the emergence of RNA-targeted agents, antibodies, and analogues that precisely modulate these pathways.
ApoCIII inhibitors like olezarsen are already approved for severe hypertriglyceridemia. ANGPTL3 inhibitors like evinacumab have shown promise in rare lipid disorders. And FGF-21 analogues like efruxifermin offer a metabolic counterpunch for the liver.
These aren’t statin competitors, they’re orthogonal tools for a different class of lipid-driven disease.
Acute Pancreatitis: A Crisis of Triglyceride Overflow
When triglycerides cross the 1,000 mg/dL threshold, the risk of acute pancreatitis spikes.
Chylomicron particles clog capillaries in the pancreas, releasing toxic free fatty acids that trigger inflammation and necrosis. It’s a high-stakes, high-cost event, often requiring ICU-level care, and for decades, we’ve lacked targeted tools to prevent it.
That’s changing.
ApoCIII inhibitors have already proven effective at reducing triglycerides by 70-80% in patients with familial chylomicronemia syndrome (FCS) and severe hypertriglyceridemia. More importantly, they’ve been linked to real-world reductions in pancreatitis episodes. This is a clinical and economic win.
ANGPTL3/8 inhibition may offer a complementary path by acting on both fasting and postprandial lipids.
These regulators influence lipase activity at different timescales and tissues.
A well-calibrated combo approach could address daily fluctuations in triglyceride handling, preventing spikes that trigger pancreatitis in vulnerable patients.
Expect this use case to expand, particularly in populations that traditional fibrates and fish oils failed to protect.
Atherosclerosis: Beyond LDL, the Remnant Revolution
LDL cholesterol may be the kingpin of atherosclerosis, but remnant particles, those leftover from triglyceride-rich VLDL and chylomicrons, are gaining notoriety as co-conspirators. They’re rich in cholesterol, pro-inflammatory, and sticky to the endothelium. And unlike LDL, they’re not always cleared by statins or PCSK9 inhibitors.
That’s where LPL-activating strategies shine.
By accelerating remnant clearance, these drugs reduce atherogenic burden at a different point in the lipid cascade. Epidemiological data suggest that lifelong suppression of ApoCIII or ANGPTL3 correlates with lower cardiovascular risk, even in those with normal LDL levels.
But this is still a bet.
No major cardiovascular outcomes trial has yet proven that these agents reduce heart attacks or strokes.
The challenge is complex: identify the right patients (remnant-driven risk), design long enough trials, and prove additive benefit on top of existing lipid-lowering therapy.
If successful, we could be looking at a new class of ASCVD preventives, not for everyone, but for the millions with residual risk that LDL alone can’t explain.
MASH: The Liver as Lipid Sensor and Signal Hub
In the context of steatohepatitis, the problem isn’t just excess fat, it’s the inflammatory and fibrotic response it triggers.
FGF-21 analogues represent a novel attempt to rewire hepatic metabolism, not by directly targeting lipids, but by restoring insulin sensitivity and mitochondrial function in the liver.
Unlike LPL modulators, which act systemically and acutely, FGF-21 agents work more like chronic metabolic remodelers. They reduce de novo lipogenesis, improve β-oxidation, and downregulate inflammatory signaling. Clinical trials show clear reductions in hepatic fat content, and several agents have demonstrated fibrosis regression, something that eluded earlier NASH hopefuls.
The irony is that these agents, while metabolically active, don’t always lower plasma triglycerides as dramatically. Their success underscores a broader truth: not all triglyceride-driven diseases are created equal. In the liver, it’s not the plasma particle that matters most, but how the hepatocyte handles its internal load. FGF-21 may be less about lipase and more about load management.
ASOs: Antisense Meets Manufacturing Leverage
Modern ASOs are precise, liver-targeted, and commercially viable.
GalNAc conjugation ensures hepatocyte delivery.
Monthly dosing ensures compliance.
The regulatory path is getting smoother with every approval.
But what’s coming next is even more interesting. We’re about to see whether ASOs can make the leap from rare disease into garden-variety hypertriglyceridemia.
That’s the question behind the CORE and CORE2 readouts, two pivotal Phase 3 trials run by Ionis, evaluating olezarsen, a GalNAc-conjugated antisense inhibitor of apolipoprotein C-III (ApoCIII). The drug is already approved as Tryngolza for familial chylomicronemia syndrome (FCS), a rare genetic disorder marked by extreme triglyceride elevations and recurrent pancreatitis. But these studies target a much broader population: patients with severe hypertriglyceridemia (≥500 mg/dL) due to more common metabolic dysfunction. If the results are positive, ApoCIII inhibition will move from orphan indication to frontline lipid therapy.
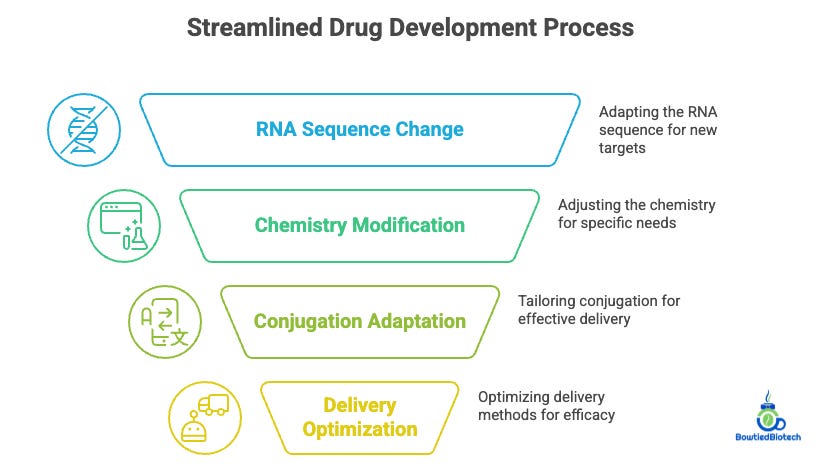
Behind olezarsen, Ionis and AstraZeneca are building modular ASO platforms where the backbone stays the same, chemistry, conjugation, delivery and only the RNA sequence changes. That allows them to rapidly pivot from ApoCIII to ANGPTL3, ANGPTL4, or future targets with the same CMC infrastructure. It’s a plug-and-play model that shrinks development timelines, lowers manufacturing risk, and gives them broad optionality across hepatic diseases.
This isn’t just about one drug. It’s about validating a format that can repeatedly deliver liver-targeted metabolic therapies with minimal reinvention—an approach that could redefine how lipid diseases are treated, trialed, and commercialized.
Most investors miss this: ASOs aren’t just drugs, they’re platforms. You don’t need to reinvent the wheel each time.
That opens the door to broad liver portfolios with lower marginal cost, faster development time, and the ability to adapt pipelines based on shifting biology or payer preferences.
Gene Editing: One Shot, One Future
Lilly’s $1B acquisition of Verve wasn’t a fluke—it was a flag in the ground. Editing is here, and it’s serious. VERVE-102, targeting PCSK9, is showing durable ~55% LDL-C reductions from a single dose. VERVE-201 aims at ANGPTL3 to lower remnants and Lp(a) simultaneously.
These aren’t incremental drugs. They’re replacements for chronic therapy.
Editing has a steep bar to clear (safety, off-target risk, delivery) but the upside is transformational. What statins do over 20 years, an editor could do in 20 minutes. And as cardiac-specific delivery matures, the potential shifts from blood lipid modulation to direct plaque remodeling, macrophage reprogramming, and vascular rejuvenation.
Don’t be surprised if the first muscle- or heart-directed CRISPR base editor hits the clinic before 2027. Academic groups are already working on this. The long game? Edit once, treat forever, and eliminate risk at its root.
Immune-Lipid Convergence: The Athero-Inflammatory Link
CANTOS taught us that inflammation matters. Blocking IL-1β reduced cardiovascular events independent of LDL-C. More recent work shows that immune checkpoints like PD-1 and CTLA-4 are active inside plaques, meaning we can modulate the immune tone of atherosclerosis, not just lipid content.
This opens up fascinating combinations:
PCSK9 editing plus low-dose IL-6 blockade to address residual inflammatory risk.
ApoCIII inhibition plus CD47-based macrophage reprogramming to clear necrotic cores.
These combos won’t show up in LDL curves, they’ll show up in plaque stability, efferocytosis, and long-term event rates.
If trials shift endpoints toward imaging and systems biology, we could see next-gen cardiometabolic regimens that blend lipid control and immune modulation in the same way oncology blends cytotoxic and checkpoint strategies.
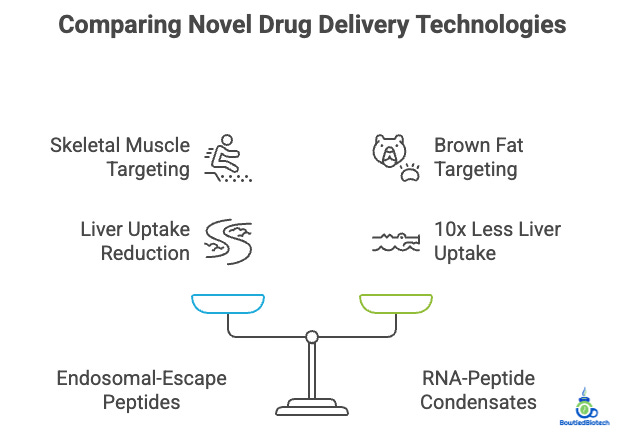
Beyond the Liver: Delivery’s New Frontier
All of this depends on delivery. Right now, everything hits the liver. But LPL biology lives elsewhere, skeletal muscle, adipose, even the heart.
Two technologies are quietly shifting the map:
Endosomal-escape peptides are enabling skeletal muscle targeting in primates.
Self-assembling RNA-peptide condensates are steering payloads to brown fat with 10x less liver uptake.
These aren’t big pharma plays yet, they’re academic or stealth biotech bets. But they could open the door to editing in tissues that have long been out of reach.
Once that unlock happens, editing isn’t just a liver story, it’s a whole-body metabolic rewiring strategy. And the companies who see that early will be the ones building the next dominant platforms.
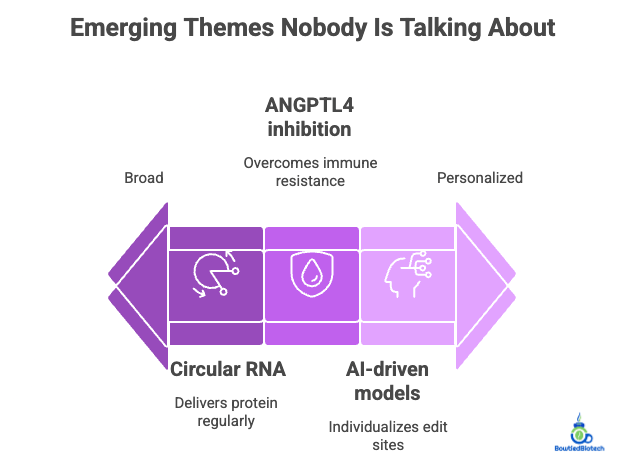
Wildcards: What Everyone Else Misses
Several themes are hiding in plain sight.
ANGPTL4 inhibition may have crossover benefits in oncology, particularly in lipid-rich tumors where immune resistance is high.
Circular RNA platforms could deliver LPL or ANGPTL3 protein every six months with a single injection, undercutting both ASOs and mRNA.
And AI-driven “digital twin” lipid models could individualize edit sites and dosing schedules based on real-time lipidomic and immune data.
None of these are priced in. All of them are being quietly developed. And they’ll likely define the next leap in metabolic therapy, not with new targets, but with new ways to match target, tissue, and patient.
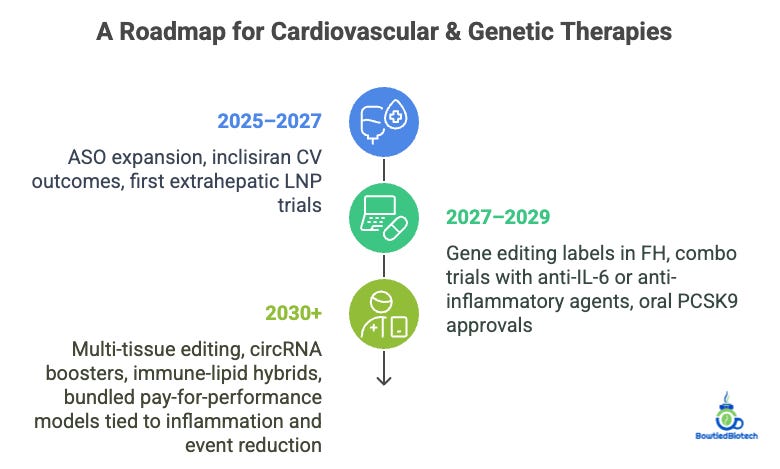
Translation Blueprint: What Comes Next
For fun we thought we would project how this all stacks up over time:
Short-term (2025–2027):
ASO expansion, inclisiran CV outcomes, first extrahepatic LNP trials.
Mid-term (2027–2029):
Gene editing labels in FH, combo trials with anti-IL-6 or anti-inflammatory agents, oral PCSK9 approvals.
Long-term (2030+):
Multi-tissue editing, circRNA boosters, immune-lipid hybrids, bundled pay-for-performance models tied to inflammation and event reduction.
The future is looking bright!
What the Trials Don’t Tell You Yet
New technology is always fun to talk about, but lets shift to where it must be proven out - in the clinic. So far, most of the excitement has been biochemical - large reductions in triglycerides, cleaner remnant profiles, and early signs of reduced organ stress.
But the leap from lipids to lives saved is nontrivial.
Most of these programs remain in Phase 2, and only a few have crossed the regulatory finish line in niche indications.
We still don’t know who benefits most:
Is it the patient with baseline triglycerides of 300?
Or the one with genetic defects in LPL regulation?
What’s the added value if you’re already on a statin and GLP-1?
These questions aren’t just academic, they determine payer uptake, trial design, and ultimately, whether these drugs become niche tools or foundational therapies.
The next wave of trials must stratify patients not just by lipids, but by end-organ vulnerability.
A pancreatitis patient has different needs than a MASH patient, and cardiovascular risk reduction is its own beast entirely. Smart design will mean layering biomarkers, imaging, and functional outcomes, not just relying on triglyceride drop as the north star.
Strategic Implications for Biotech and Pharma
This shift toward LPL-enhancing therapeutics opens new strategic lanes for drug developers.
Companies that once competed in silos (liver disease, lipidology, endocrinology) now find themselves circling the same biology. That convergence creates both M&A opportunity and internal portfolio conflicts.
For platform companies, the challenge is proving that these are not one-trick assets. Can a single molecule straddle multiple indications and geographies? Can it scale from rare disease to broad cardiometabolic populations without losing efficacy or payer support?
For pharma, the question is timing. Outcomes trials take years, but if you wait for those to read out, the best assets may be gone.
We expect the most aggressive acquirers to be those with large metabolic franchises and unmet pipeline gaps, Novo Nordisk, Amgen, Lilly, and possibly Pfizer. Those with both GLP-1 and NASH ambitions have the most to gain from a diversified lipid play. It’s a question of complement, not cannibalization.
Why This Matters Now
The field isn’t about picking a single horse anymore. It’s about stacking optionality (ASOs, editing, immune modulators, targeted delivery) and building adaptive platforms that move with biology, not against it.
The winners won’t be those who lower lipids the most. They’ll be those who understand lipid logic, the networks, the nodes, and the new ways to intervene.
The urgency here isn’t theoretical.
Acute pancreatitis admissions are rising.
Cardiovascular risk remains stubbornly high despite LDL control.
MASH is now the leading cause of liver transplantation in the U.S.
The common thread? Lipid mismanagement, not just cholesterol, but the entire cascade of remnant, triglyceride, and hepatic lipid flux.
We’re entering a new phase in metabolic medicine, one that requires a different lens. This isn’t about dieting patients into lower LDL or running ever-larger statin trials. It’s about targeting lipid handling at the source, via enzymes like LPL and hormonal networks like FGF-21. The tools exist. The biology is clear. What remains is the will to invest in smarter trial design and longer-term thinking.
It’s no coincidence that multiple biotech firms are converging here at once. The same way PCSK9 changed the LDL story, this class could reshape the next generation of cardiovascular and metabolic disease therapeutics, if the data keep pace.
CONCLUSION
Today, investors and operators alike face a clear decision point. The science behind triglyceride-lowering and LPL-enhancing drugs is mature, the mechanisms are validated, and regulatory traction is building. What remains is clarity on where the biggest wins will be (pancreas, heart, or liver) and which programs will generate the outcomes data to unlock broader adoption. As the metabolic map expands, the next dominant players will be those who move early, align biology with strategy, and build across indications, not just within them.
As a reminder, if looking to go deeper into the topics we cover check out our website BowTiedBiotech.com, or DM us on twitter, or email us: bowtiedbiotech@gmail.com
DISCLAIMER
None of this is to be deemed legal or financial advice of any kind. All updates are sourced from publicly available disclosures. Insights are *opinions* written by an anonymous cartoon/scientist/investor.
TOP BOWTIEDBIOTECH NEWSLETTERS